A car crash can end in a strange way. The airbags go off, the police arrive, the tow truck leaves, and someone in your family says, “I think I'm okay.” Then the next morning comes. The headache won't quit. Bright light feels harsh. Words are harder to find. A simple conversation feels like work.
That gap between “I survived” and “something still isn't right” is where many families get lost.
A traumatic brain injury screening is often the first step that helps make sense of that feeling. It can point doctors toward the right follow-up care, and it can also create a medical record that matters later if the crash leads to an insurance claim or lawsuit. When a brain injury doesn't show up as a cast, a bruise, or a dramatic scan result in the emergency room, families need a clearer way to explain what changed and when it changed.
The Invisible Injury After a Crash
Maria gets rear-ended at a stoplight. She walks out of the car. She talks to the officer. At the emergency room, she answers questions, moves her arms and legs, and goes home relieved that nothing seems broken.
Two days later, she starts forgetting why she opened the refrigerator. She loses track of a sentence halfway through saying it. Her neck hurts, but what scares her more is the fog. Her husband notices she's snapping at the kids and then crying because she can't explain what's wrong.
That story is common after a crash. A brain injury can be real, disruptive, and medically important even when there's no cut on the head and no dramatic finding right away.

Why families often miss it
After a collision, adrenaline can hide symptoms. People focus on obvious injuries first. Emergency rooms also have a hard job. They look for immediate dangers, such as bleeding, fractures, or life-threatening changes in consciousness. If those emergencies aren't present, a person may still leave with a brain that isn't functioning normally.
That's why people call TBI an invisible injury. You may look normal to others while feeling unlike yourself inside.
What screening does
A traumatic brain injury screening is not magic, and it isn't a final diagnosis by itself. It's more like turning on a flashlight in a dark room. It helps a clinician ask the right questions about the crash, your symptoms, your memory, your balance, and the way your brain is working in everyday tasks.
Practical rule: If someone feels mentally, emotionally, or physically “off” after a crash, don't wait for visible proof before asking for a brain injury screening.
This matters globally, not just in one hospital or one city. In 2021, there were 20,837,466 new cases of traumatic brain injury worldwide, and 56.63% were classified as moderate or severe, according to a Frontiers in Public Health article on global TBI burden and screening. That same source notes that because TBI often presents without visible external signs, systematic screening is critical.
For a family after a crash, the takeaway is simple. If the person you love seems different, treat that change seriously. The screening is often the first paper trail for health, recovery, and accountability.
Recognizing the Symptoms That Warrant Screening
Some people expect a brain injury to look dramatic. Loss of consciousness. Slurred speech. Collapse. Sometimes it does. Often it doesn't.
A lot of post-crash TBIs show up in quieter ways. Someone says, “I just can't focus,” or “I feel weird,” or “I'm exhausted but I can't sleep.” Those symptoms are enough to justify asking for evaluation.
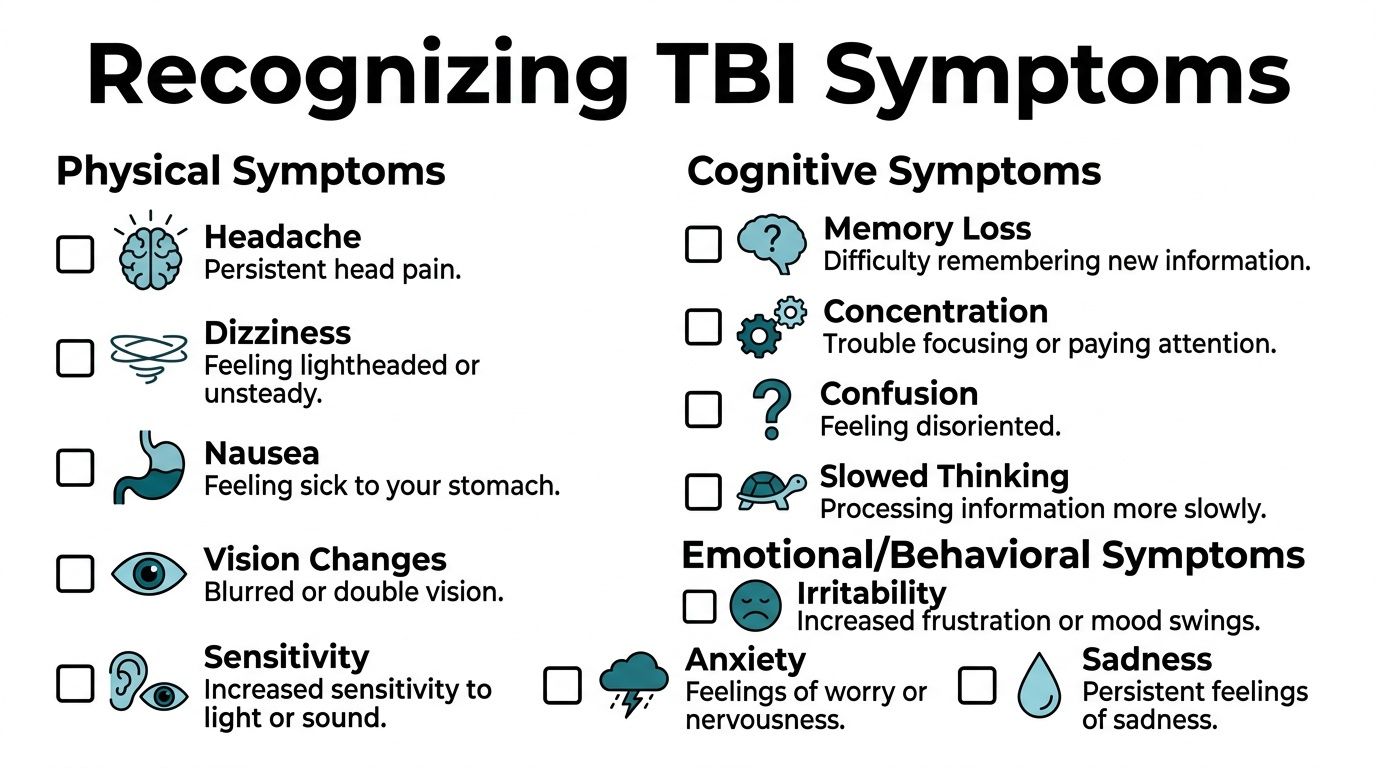
Physical signs
Look for symptoms that involve the body's basic systems:
- Head pain: A headache that starts after the crash, gets worse, or keeps returning.
- Dizziness: Feeling lightheaded, unsteady, or like the room is moving.
- Nausea: An unsettled stomach, especially when paired with head pain or dizziness.
- Vision changes: Blurry vision, double vision, or trouble focusing.
- Sensitivity: Light and sound suddenly feel harsher than usual.
- Balance trouble: Walking feels awkward, or turning quickly makes symptoms flare.
Cognitive signs
These symptoms often create the most confusion because they can sound vague:
- Memory problems: Forgetting recent conversations, appointments, or simple tasks.
- Brain fog: Feeling slowed down, disconnected, or mentally cloudy.
- Trouble concentrating: Reading the same sentence several times or losing track mid-task.
- Confusion: Difficulty following directions or processing information that used to feel easy.
- Word-finding trouble: Knowing what you want to say but not being able to say it smoothly.
Families often first notice these changes during ordinary routines, not in the doctor's office.
You can also learn more about how memory issues can fit into a post-impact brain injury picture in this guide on memory loss after head trauma.
A short visual explanation may help if you're trying to compare symptoms with what you've seen at home.
Emotional and behavioral signs
Brain injuries can affect mood and stress tolerance. That doesn't mean the person is “just emotional.”
- Irritability: Short temper, frustration, or sudden anger that seems out of character.
- Anxiety: A new sense of panic, nervousness, or overwhelm.
- Sadness: Tearfulness or a flat, low mood after the impact.
- Sleep changes: Sleeping too much, sleeping too little, or waking often.
- Overstimulation: Crowds, screens, noise, or busy places feel unbearable.
A person doesn't need to lose consciousness for a brain injury to be worth screening.
The risk after head trauma is high enough that mild-looking incidents shouldn't be brushed off. In a study of adults admitted from emergency departments, 57.5% of those with head trauma were diagnosed with a TBI, and males are three times more likely to die from a TBI than females, according to the CDC's traumatic brain injury data page.
If several symptoms appeared after a crash, or one symptom keeps lingering, that's usually reason enough to ask for screening.
What to Expect During a TBI Screening
Many families hear the word “screening” and picture a single pass-fail test. That's not usually how it works. A traumatic brain injury screening is more like a clinician gathering clues.
Think of it as a careful interview plus a set of simple checks. The provider is trying to answer a practical question: Is this person's brain functioning differently after the crash?
The conversation comes first
The appointment often starts with the story of the crash. The clinician may ask:
- what happened during the impact
- whether the head struck anything
- whether there was a sudden whip-like movement
- what symptoms started right away
- what symptoms showed up later
- whether there have been prior head injuries
That history matters. The details often explain why someone feels fine in one setting but struggles in another.
Simple tasks, not trick questions
After the history, the provider may check short-term memory, attention, eye movement, reaction, or balance. That can include remembering a few words, following a sequence, standing steadily, or describing symptoms in plain language.
These tasks can feel almost too simple. Families sometimes wonder how repeating words or walking in a straight line could reveal anything important. The answer is that subtle problems with attention, coordination, and processing often appear during ordinary tasks before they show up anywhere else.
If you freeze during screening or forget details, that doesn't mean you've failed. It gives the clinician useful information.
Why follow-up mental health evaluation can matter
A crash can affect more than cognition. Sleep, anxiety, mood swings, fear of driving, and stress can all mix with brain injury symptoms. If a provider recommends a broader behavioral or emotional assessment, families may find it helpful to understand the reVIBE Mental Health evaluation process so they know what a structured mental health evaluation looks like and how it fits into overall care.
That kind of follow-up doesn't replace TBI screening. It complements it when symptoms overlap.
What screening is not
It helps to clear up three common misunderstandings.
| Misunderstanding | More accurate view |
|---|---|
| “The screening will diagnose everything.” | Screening flags concerns and helps decide what should happen next. |
| “If I can answer questions, my brain must be fine.” | Many people with TBI can hold a conversation while still having significant deficits. |
| “A normal first exam ends the matter.” | Symptoms can evolve, and a later, more targeted evaluation may reveal problems the first visit didn't catch. |
The goal is not to trap you. The goal is to see the injury more clearly so treatment decisions can be made on something firmer than guesswork.
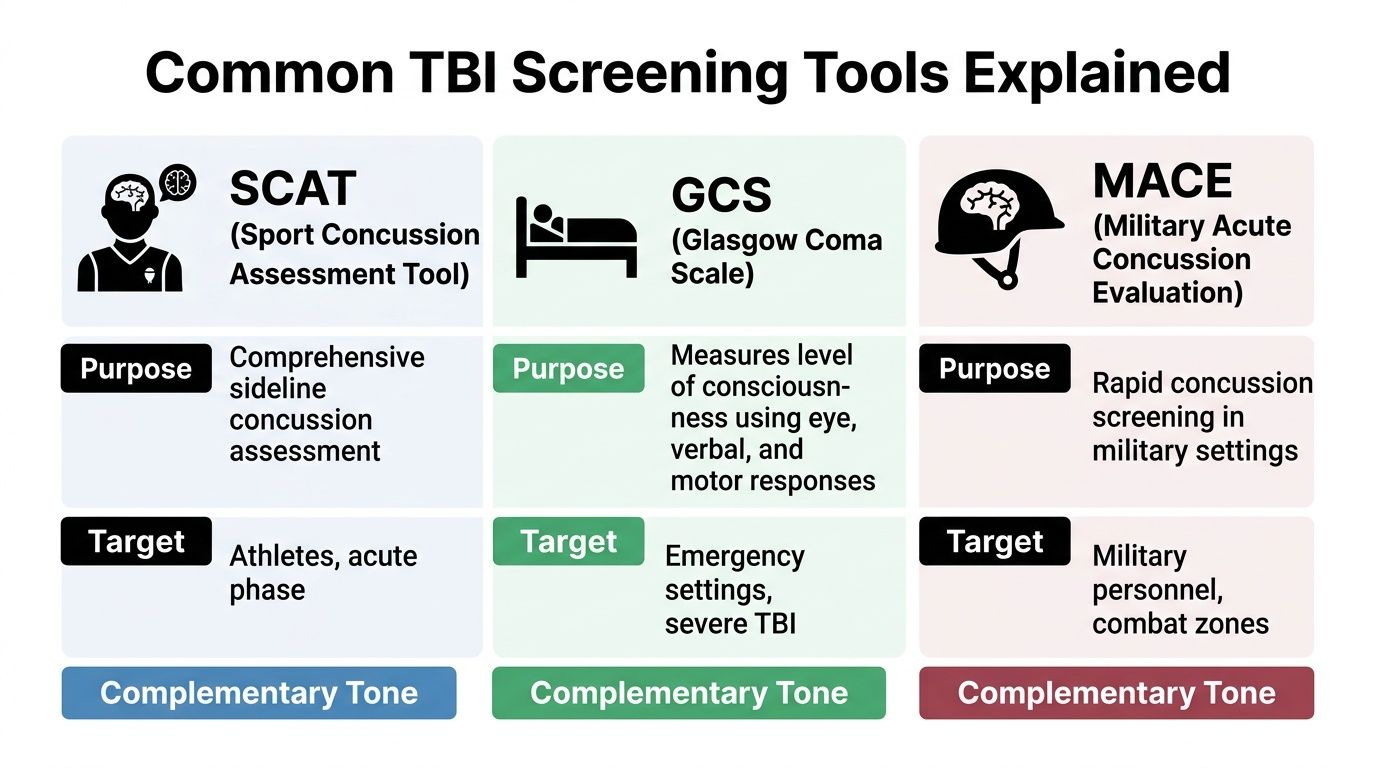
Common TBI Screening Tools Explained
The names of these tools can sound like alphabet soup. SCAT. GCS. MACE. ACE. OSU TBI-ID. HELPS. BISQ. Families often assume they all do the same thing. They don't.
Each tool has a different job, a different setting, and different strengths. Some are fast checks. Some are structured interviews. Some work better in sports, some in hospitals, and some in long-term follow-up.
Quick tools used in the moment
SCAT
The Sport Concussion Assessment Tool is commonly used around sports-related injuries. It's designed for an acute setting, often close in time to the injury, and it includes symptom checks along with tasks involving concentration and balance.
GCS
The Glasgow Coma Scale is widely used in emergency care. It looks at eye, verbal, and motor responses to help assess consciousness. It's useful, especially in more serious trauma, but it does not answer every question about subtle post-crash brain dysfunction.
MACE
The Military Acute Concussion Evaluation is associated with military and combat settings. It is built for rapid concussion screening where quick decisions matter.
Clinical tools used beyond the first moment
ACE
The Acute Concussion Evaluation is a clinical checklist often used by physicians to organize symptoms, injury details, and follow-up concerns in a more structured way.
ImPACT
This is a computerized neurocognitive testing tool often discussed in sports and return-to-activity settings. It can help compare thinking skills over time.
These tools can be useful, but they aren't interchangeable. A sideline sports tool is not the same as a deeper retrospective interview for someone weeks or months out from a car crash.
Tools designed to catch what brief screens miss
Families often run into trouble because a short screen, while helpful, can also miss injuries.
The OSU TBI-ID is a structured, validated self-report tool designed for retrospective lifetime exposure identification in the general population, and the source describing global screening needs notes it is recommended for use in direct service settings because it helps ensure cases aren't missed, as described in the earlier linked global burden source.
The BISQ, or Brain Injury Screening Questionnaire, is another structured self-report tool that covers TBI history, symptoms, and other health conditions. It's especially valuable because it helps uncover cases that may never have been documented in emergency settings.
Some tools require more detailed prompting. The HELPS screen can be important when injuries stem from falls, assaults, abuse, or repeated impacts and the person doesn't immediately connect those events to a brain injury.
If you've been told a provider may order more formal testing after a screen, this overview of neurological tests for brain damage can help you understand how screening fits into the wider evaluation process.
Why “brief” doesn't always mean “enough”
A short screening tool can be a useful doorway. It just shouldn't always be the last word.
The problem is sensitivity. Some brief tools miss people who really do have a history of brain injury. In one study, the TBI-4 failed to identify 36% of veterans with a confirmed TBI history, which is why more detailed structured interviews like the OSU TBI-ID are often necessary for accurate diagnosis, according to the American Journal of Public Health article on TBI screening sensitivity.
Key distinction: A quick screen is good for raising concern. A structured interview is better for understanding the full injury history.
That distinction matters in medical care. It also matters when an insurance adjuster later argues that no one documented the brain injury early enough.
How Screening Results Guide Your Next Steps
A screening result is best understood as a fork in the road. It tells the care team whether to keep watching, to look deeper, or to act quickly.
A positive screen does not mean “final diagnosis reached.” It means there are enough concerns to justify more focused evaluation. That is good news in one sense. It opens doors to care that families often need.
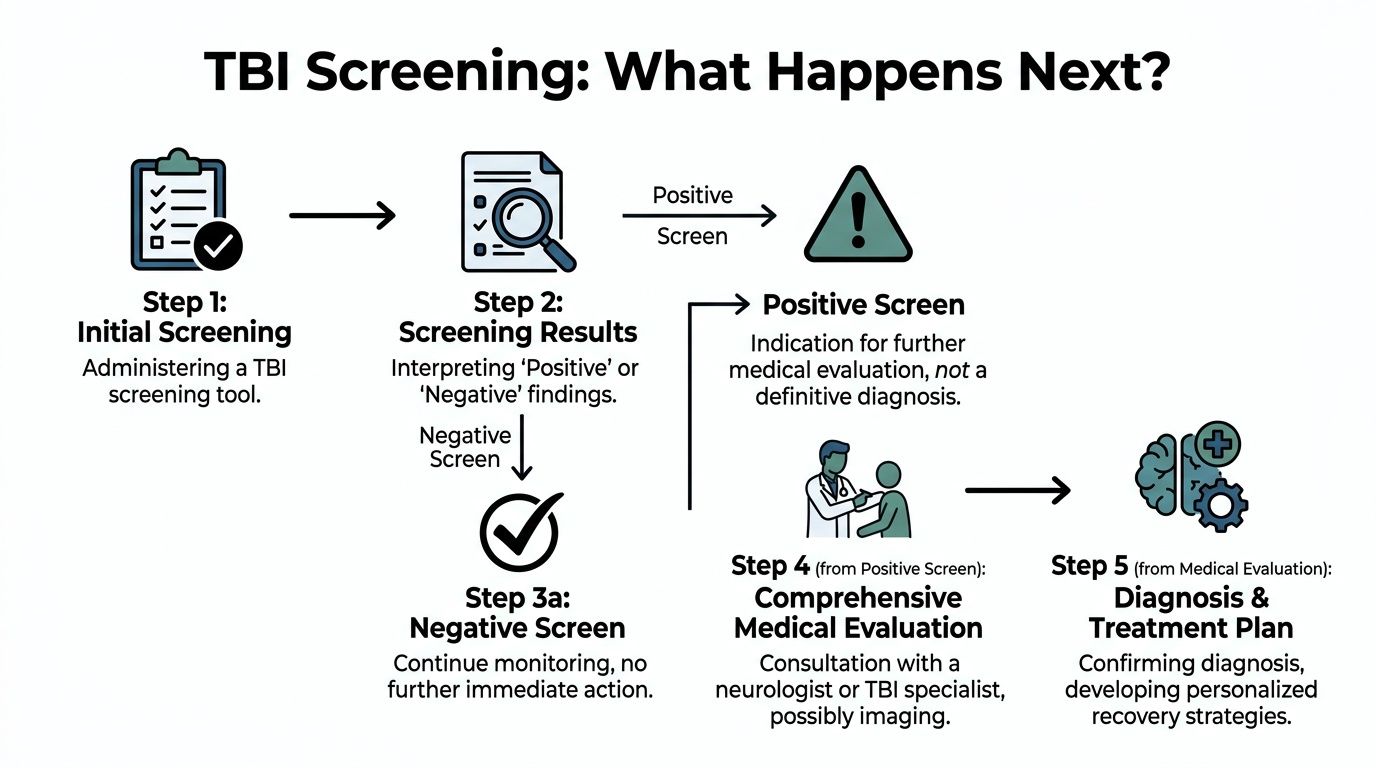
If the screen raises concern
The next steps may include:
- Specialist referral: A neurologist, neuropsychologist, physiatrist, or concussion specialist may do more detailed testing.
- Imaging when appropriate: A doctor may order CT or MRI to look for structural issues, depending on the situation.
- Symptom management: The patient may receive guidance about rest, activity limits, screen use, sleep, headache care, and follow-up timing.
- Monitoring over time: Repeat assessment can matter because some deficits become clearer after the immediate chaos of the crash fades.
If the screen is less concerning
A less concerning screen doesn't always end the matter. A clinician may still tell the family to watch for worsening headaches, vomiting, confusion, new balance problems, mood changes, or persistent cognitive trouble.
That's because brain injuries don't always announce themselves on the first day.
Why the full picture matters
Modern TBI care is moving away from judging the injury by symptoms alone. A newly proposed framework called CBI-M uses four pillars: clinical presentation, biomarkers, imaging (CT/MRI), and modifiers such as injury mechanism and other contextual factors, creating a more precise and personalized recovery plan, according to the Brain Injury Association of America summary of the CBI-M classification framework.
That framework is useful for families because it mirrors real life. Two people can have similar headaches after a crash but very different recovery paths depending on how the injury happened, whether they had a prior TBI, what imaging shows, and what stressors affect their healing.
What you should keep at home
After a screening, families should start building a simple record.
- A symptom journal: Note headaches, memory slips, fatigue, mood changes, and sleep disruption.
- Appointment records: Save discharge paperwork, referrals, and follow-up recommendations.
- Work and school effects: Write down missed days, reduced hours, or struggles with routine tasks.
Those details help doctors adjust care. They also become useful evidence if legal questions arise later.
Why Screening Documentation Is Critical for Your Legal Claim
Insurance companies often look for gaps. If there's a delay in treatment, they may say the injury wasn't serious. If the ER note says “alert and oriented,” they may argue there was no brain injury at all. If symptoms weren't documented early, they may claim the problems came from stress, age, or something unrelated.
That's why screening documentation matters so much.
The medical record becomes evidence
A timely traumatic brain injury screening creates a record of what the patient reported, what the clinician observed, and what concerns existed close to the crash. That record can show:
- Symptom timing: When headaches, fogginess, memory problems, or balance issues began.
- Functional changes: Trouble concentrating, sleeping, working, driving, or managing routine tasks.
- Need for follow-up care: Referrals, monitoring, and additional evaluation were medically justified.
Without that paper trail, families often end up trying to prove a brain injury months later with memories alone.
Why proactive screening closes a dangerous gap
Systematic screening with tools like the BISQ uncovers a much higher rate of TBI than previously estimated, showing that many cases go undocumented without proactive screening. That gap matters for public health and for legal documentation, as described in the BISQ research article in PubMed Central.
For a legal claim, undocumented symptoms are a problem. Not because they aren't real, but because insurers often pretend that what isn't written down didn't happen.
A good legal case usually starts with good medical documentation.
Keep records private, organized, and complete
Families often need to store imaging reports, symptom journals, discharge papers, work notes, and copies of correspondence. If you need to convert or organize those materials digitally, a privacy-focused tool such as File Studio for private conversions can be useful when handling sensitive medical files.
Preservation matters too. Photos of the vehicle, black box data when available, medical paperwork, and electronic records can all become important pieces of the case. If you're worried about lost or destroyed evidence, this explanation of what spoliation of evidence means gives a plain-language overview of why early preservation steps matter.
The legal point is straightforward. Screening is not only about getting help. It's also about making sure the injury exists in the record before someone else tries to erase it with doubt.
Frequently Asked Questions About TBI Screening
What if the ER doctor said I was fine but I still feel off
That happens often. Emergency care focuses first on immediate danger. A person can leave the ER without a crisis finding and still have a brain injury affecting memory, mood, attention, sleep, or balance.
If symptoms continue, ask for follow-up evaluation. Write down what has changed since the crash. Bring a family member if possible, because loved ones often notice changes the injured person can't easily describe.
Can a screening tool detect old or multiple brain injuries
Sometimes, but only if the questions are detailed enough. People often get tripped up on this very condition.
Some screening tools require specific prompts about falls, assaults, or abuse to uncover injuries a person may forget or never label as brain injuries. Guidance also recommends such tools in detecting TBI related to domestic violence, a context standard intake often misses, according to New Mexico Brain Injury Advisory Council guidance on the HELPS screening tool.
That means a rushed intake form may not tell the full story. If someone has had more than one head impact, or injuries from violence at home, the provider needs to ask carefully and specifically.
Does a negative screen mean nothing is wrong
Not always. It may mean no clear concern was found at that moment, or it may mean the screening tool was limited. If symptoms persist, worsen, or interfere with work, school, parenting, or driving, follow up anyway.
A negative first screen should never outweigh lived symptoms that continue to disrupt daily life.
How much does TBI screening cost and will insurance cover it
Coverage depends on the provider, the setting, the kind of screening, and the insurance plan. Some screenings happen as part of a regular medical visit. Others are folded into specialist evaluation. The practical step is to ask two questions before the appointment:
- What kind of provider is doing the screening
- How will the visit be billed
If the crash involved someone else's negligence, keep receipts, bills, and mileage records related to care.
What should I bring to the appointment
A short list helps:
- Crash details: Date, time, and a simple description of what happened.
- Symptom timeline: What started immediately and what appeared later.
- Medication list: Include anything new taken after the crash.
- Witness observations: Notes from a spouse, friend, or coworker who saw changes.
- Prior history: Any earlier head injuries, migraines, learning issues, or mental health treatment.
Where can families find reputable help
Start with clinicians experienced in concussion and TBI care. National advocacy organizations can also help families find education and support, including the Brain Injury Association of America and government public health resources on traumatic brain injury.
The most important thing to remember is this: if your loved one is not acting like themselves after a crash, trust that observation and get it documented. Families are often the first ones to see the truth of a brain injury.
If your family is dealing with fogginess, headaches, memory changes, or other post-crash symptoms, Nares Law Group LLC can help you understand the legal side while you focus on medical care. The firm represents people harmed in motor vehicle and truck crashes, including cases involving traumatic brain injuries, and works to protect the documentation, evidence, and rights that can shape your future.