You went to the emergency room after a crash, a fall, or a blow to the head. The CT scan was called “normal.” Then you went home and discovered that normal didn't feel normal at all.
Now you're dealing with headaches, brain fog, memory slips, dizziness, irritability, sleep problems, or a strange sense that your brain just doesn't work the way it did before. Family members may notice it. Coworkers may notice it. But on paper, the first scan looks clean.
That gap is where many traumatic brain injury cases become both medically confusing and legally difficult. A traumatic brain injury MRI often helps close that gap. It can reveal injuries a CT scan was never designed to show, and when it does, that scan can become critical evidence in a personal injury claim.
Your TBI Symptoms Are Real Even if Your CT Scan Is Normal
A normal CT scan often gets treated like the end of the story. For many people, it's only the first chapter.
CT scans are built for emergencies. In the hours right after a head injury, doctors use them to quickly look for major bleeding, dangerous swelling, or skull fractures. That makes sense in an ER. If someone needs urgent surgery, speed matters.
But many people with mild traumatic brain injury leave the hospital still feeling unwell. They can't focus. They forget appointments. Noise feels sharper. Driving becomes stressful. They may look fine to others while struggling through each day.
A normal emergency scan can rule out a crisis without ruling out a brain injury.
That distinction matters. The symptoms can be real even when the first imaging test doesn't show the reason clearly. For a plain-language explanation of that first test, see this guide on a TBI CT scan and what it can miss.
Why this happens
The brain is soft tissue. Many traumatic brain injuries involve subtle damage to brain tissue, nerve fibers, or tiny blood vessels. CT is excellent for fast triage, but it often misses those quieter injuries.
MRI serves a different role. It gives doctors a much more detailed look at the brain itself, not just the emergency conditions around it. In a legal case, that difference can be essential. Insurance companies often lean hard on the phrase “normal CT,” even though that phrase may only mean there was no large bleed visible at the time.
What this means for your claim
If your symptoms continued after a normal CT, you're not being unreasonable by asking for more answers. You're responding to a common problem in brain injury cases.
From a legal perspective, the issue isn't just whether you were scanned. It's whether the right scan was used for the kind of injury you may have suffered. That is often where MRI enters the picture.
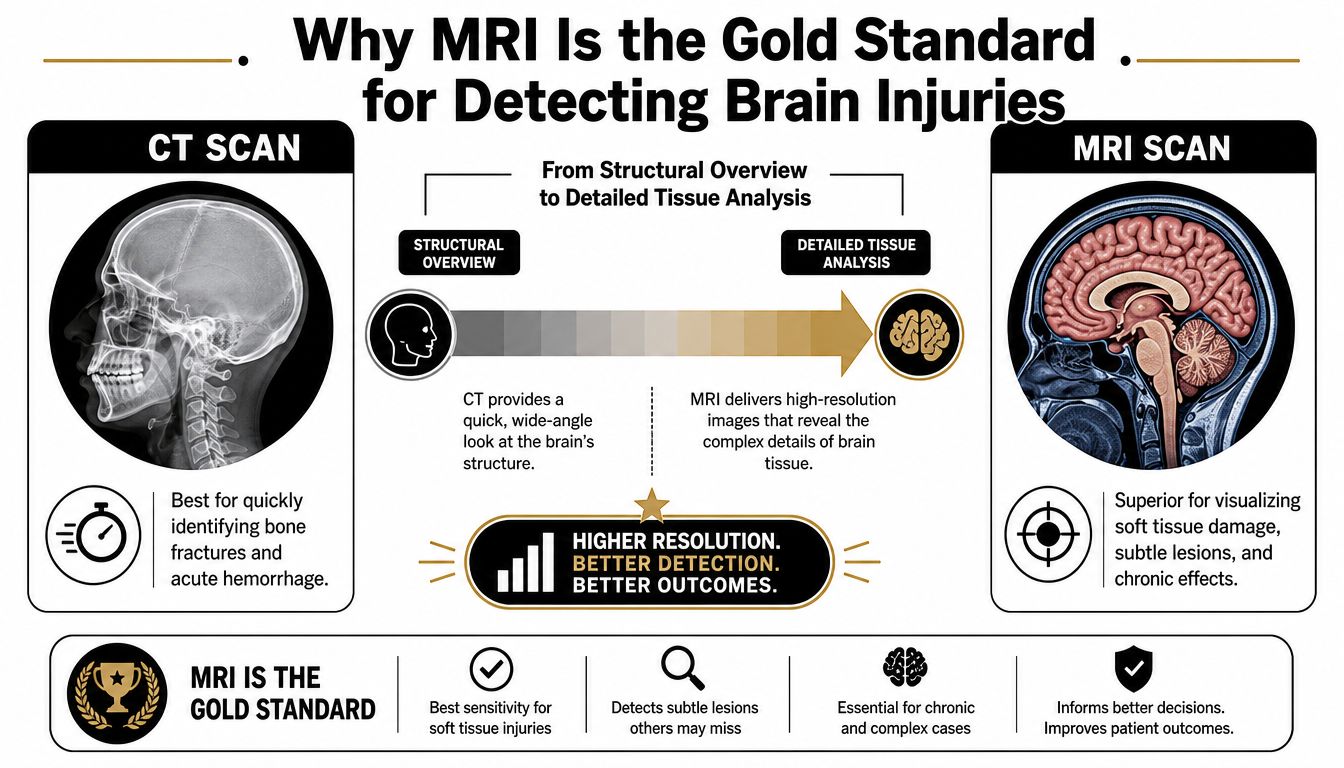
Why MRI Is the Gold Standard for Detecting Brain Injuries
Think of CT as a fast black-and-white sketch. Think of MRI as a layered high-resolution map.
A CT scan can quickly show the big, urgent problems. An MRI can show the brain's soft tissues in much greater detail. That matters because many traumatic brain injuries are not dramatic on first presentation. They are subtle, scattered, and easy to miss unless the imaging method is sensitive enough to find them.
What MRI can detect that CT often misses
MRI is especially important for injuries such as diffuse axonal injury, nonhemorrhagic contusions, brainstem injury, and white matter damage. These are the kinds of injuries that can disrupt thinking, memory, attention, mood, and coordination even when a CT scan looks unremarkable.
The difference is not just theoretical. In a study of suspected mild traumatic brain injury patients whose CT scans were negative, 9 of 19 patients, or 47%, had trauma-related abnormalities on MRI, and MRI detected diffuse axonal injury in 30% of patients with mild head injury whose CT scans were normal, as reported in this study on MRI findings after negative CT in mild traumatic brain injury.
Why insurers often get this wrong
Insurance adjusters like clean lines. They prefer arguments that sound simple. “Your CT was normal, so your brain injury must be minor or nonexistent” is one of those arguments.
The medical reality is more complicated.
| Imaging tool | Best use | Common limitation in TBI |
|---|---|---|
| CT | Fast emergency screening for fractures and major bleeding | May miss subtle soft tissue injury |
| MRI | Detailed evaluation of brain tissue and injury patterns | Usually takes longer and is not always done immediately |
A traumatic brain injury MRI matters because it answers a different question. CT asks, “Is there an emergency we must act on right now?” MRI asks, “What happened to the brain tissue?”
Practical rule: If symptoms continue but the CT was normal, it's reasonable to ask whether MRI is needed to evaluate injuries CT often misses.
Why lawyers care about this distinction
In a personal injury claim, objective evidence carries weight. MRI can transform the conversation from “the patient reports symptoms” to “the imaging shows structural findings consistent with trauma.”
That doesn't guarantee a fair outcome, but it changes the terrain. It gives your doctors stronger diagnostic support and gives your attorney a better way to challenge a denial based on a normal CT alone.
A Guide to Key MRI Sequences in TBI Diagnosis
MRI reports can look like alphabet soup. T1. T2. FLAIR. DWI. SWI. GRE. Most patients read those terms and feel lost.
You don't need to become a radiologist. But it helps to understand what these sequences are doing, because each one is trying to reveal a different type of injury.
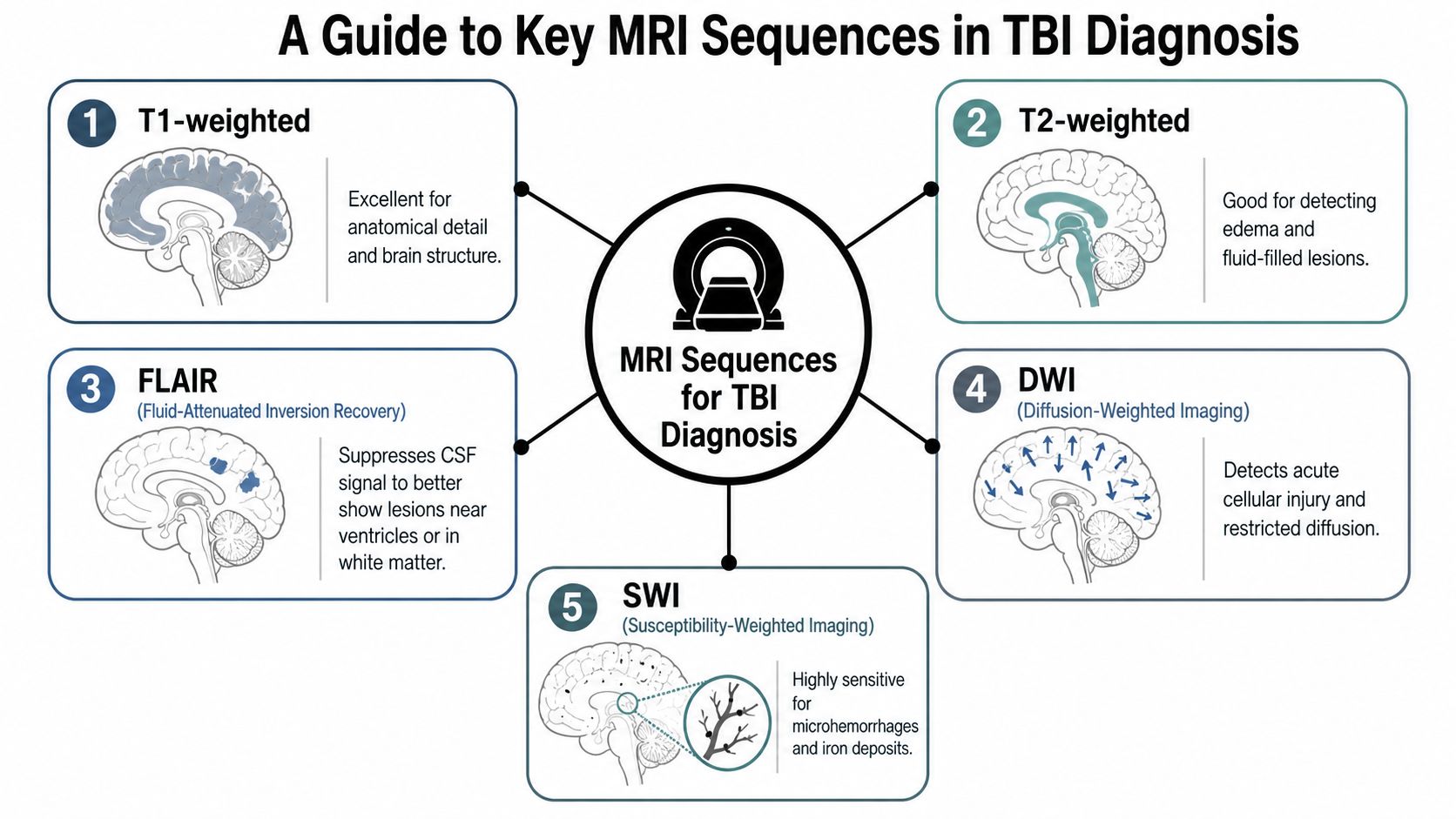
T1 and T2 give the structural map
T1-weighted images are strong for anatomy. They help show the brain's overall structure and can help identify changes in shape or volume.
T2-weighted images are better at showing fluid and edema. If tissue is holding extra water after an injury, T2 can help bring that into view.
Together, these sequences are like the base map in a case file. They show the terrain before you start highlighting the damage.
FLAIR acts like a highlighter
FLAIR stands for Fluid-Attenuated Inversion Recovery. The simplest way to think about it is this: it suppresses bright fluid signals that would otherwise distract from nearby abnormalities.
That helps radiologists spot lesions and trauma-related changes more clearly. In the mild traumatic brain injury study discussed earlier, abnormalities were most frequently identified on postcontrast FLAIR sequences.
DWI looks for acute cellular distress
Diffusion-weighted imaging, or DWI, tracks water movement in tissue. When cells are injured, water movement can change. DWI helps detect that disruption.
A useful analogy is traffic. In healthy tissue, water moves along expected paths. In injured tissue, that movement can become restricted or disorganized. DWI helps reveal where normal flow has broken down.
For readers who want a deeper legal and medical overview of advanced white matter imaging, this page on diffusion tensor imaging of the brain is a helpful companion.
SWI is the microbleed detector
Susceptibility-weighted imaging, or SWI, is especially important in traumatic brain injury. It is highly sensitive to blood products and tiny hemorrhages.
That matters because torn microscopic vessels can leave behind evidence even when larger bleeding isn't present. According to the recommended TBI imaging guidance, SWI is preferred over GRE because of its increased sensitivity for blood products, and the recommended protocol includes multiplanar T1, T2, FLAIR, and SWI or GRE for a thorough assessment, as described in this clinical MRI protocol paper for traumatic brain injury.
Why sequence choice matters in a legal case
A report that says “MRI brain normal” can hide an important question. What sequences were performed?
If the protocol was limited, the scan may not have been optimized to detect subtle traumatic findings. In litigation, that detail can matter. A defense argument built on an incomplete MRI is not as strong as it sounds if the scan didn't include the most useful sequence set for TBI evaluation.
What an MRI Reveals From Acute Injury to Chronic Effects
An MRI can tell a time-based story. It may show what happened near the injury date, and it may also show the longer shadow that injury leaves behind.

Right after trauma, radiologists may look for contusions, edema, microhemorrhages, and brainstem involvement. Later, the focus can shift toward whether the brain shows signs of lasting change, such as tissue loss, old blood product staining, or structural patterns that support ongoing symptoms.
That timeline matters in medicine because it helps doctors judge recovery and risk. It matters in a legal claim because it helps connect the initial event to long-term impairment.
Acute findings show the immediate harm
In the early stage, MRI can document the direct effects of trauma. A contusion is a bruise of the brain. Edema reflects swelling. Microhemorrhages can suggest shearing forces that affected tiny vessels and surrounding tissue.
Those findings help answer a key legal question: did this incident injure the brain?
They also help explain symptoms that seem out of proportion to a “normal” emergency workup. A patient who has slowed processing speed, imbalance, and severe fatigue may finally have imaging evidence that matches the lived experience.
Chronic findings show the injury didn't simply disappear
Months later, MRI may help show that the injury had consequences beyond the initial event. In some patients, later scans reveal patterns that support permanent or long-lasting effects.
Research has also shown that MRI findings can improve prognostic assessment. MRI measures such as total contusion volume and the presence of brainstem lesions were independently associated with long-term outcomes, and adding MRI findings improved prognostic models beyond clinical predictors alone, according to this JAMA Network Open study on MRI and TBI outcomes.
If you're trying to understand how delayed imaging can still matter, this discussion of diagnosing TBI years later is worth reading.
The biology behind long-term injury can also make more sense when you understand the brain's own brain protection mechanisms, including the blood-brain barrier. When trauma disrupts those protective systems, the effects can continue long after the accident scene is gone.
A short visual overview can help make this timeline easier to grasp:
MRI findings do not predict every outcome, but they can provide objective clues about severity, location, and the likelihood that symptoms will persist.
What to Do When Your TBI MRI Comes Back Normal
This is one of the hardest parts of a brain injury case. You finally get the MRI. You hope for answers. Then the report says “normal,” “unremarkable,” or “no acute intracranial abnormality.”
That does not automatically mean your brain is unharmed.
Conventional MRI has limits. It can miss microscopic axonal damage and other changes that affect cognition, mood, balance, and stamina. Patients often hear “normal scan” and conclude they must be imagining the problem. Insurance companies often push that same narrative because it serves their financial interest.
Why a normal MRI can coexist with real symptoms
The American Society of Neuroradiology explains this problem clearly. Over 75% of traumatic brain injuries are mild, and conventional CT or MRI in these cases often yields no specific correlation to explain cognitive and clinical symptoms, creating a gap where patients can be misled by clean scans and insurers may use those scans to deny liability, as noted in this ASNR patient guide on traumatic brain injury imaging.
That's why the right question is not just, “Was the MRI normal?” The better question is, “What kind of MRI was done, what symptoms continue, and what other clinical evidence supports the diagnosis?”
What still matters if the scan is normal
A strong brain injury case does not rest on imaging alone. Doctors also look at:
- Symptom pattern that began after the trauma and persisted over time
- Neurological examination findings
- Neuropsychological testing that shows changes in memory, attention, speed, or executive function
- Witness observations from family, friends, or coworkers who saw the before-and-after difference
- Treatment history such as vestibular therapy, cognitive rehab, headache care, or sleep treatment
“Normal” on a routine MRI may mean the injury is below the resolution of that scan, not that the patient has no injury.
How to respond without giving up
If your symptoms persist, keep treating. Keep documenting. Keep following up with providers who understand concussion and mild traumatic brain injury.
From a legal standpoint, don't let a normal MRI become the only sentence in your file. The absence of visible injury on one test is not the same as the absence of injury. That distinction often needs to be explained carefully, with medical records, symptom logs, and expert interpretation.
How MRI Evidence Strengthens Your Personal Injury Claim
A traumatic brain injury claim often turns on credibility. The defense may argue that you're exaggerating, that your symptoms are stress-related, or that a normal CT means there was no significant injury.
MRI can change that conversation because it provides objective medical evidence.
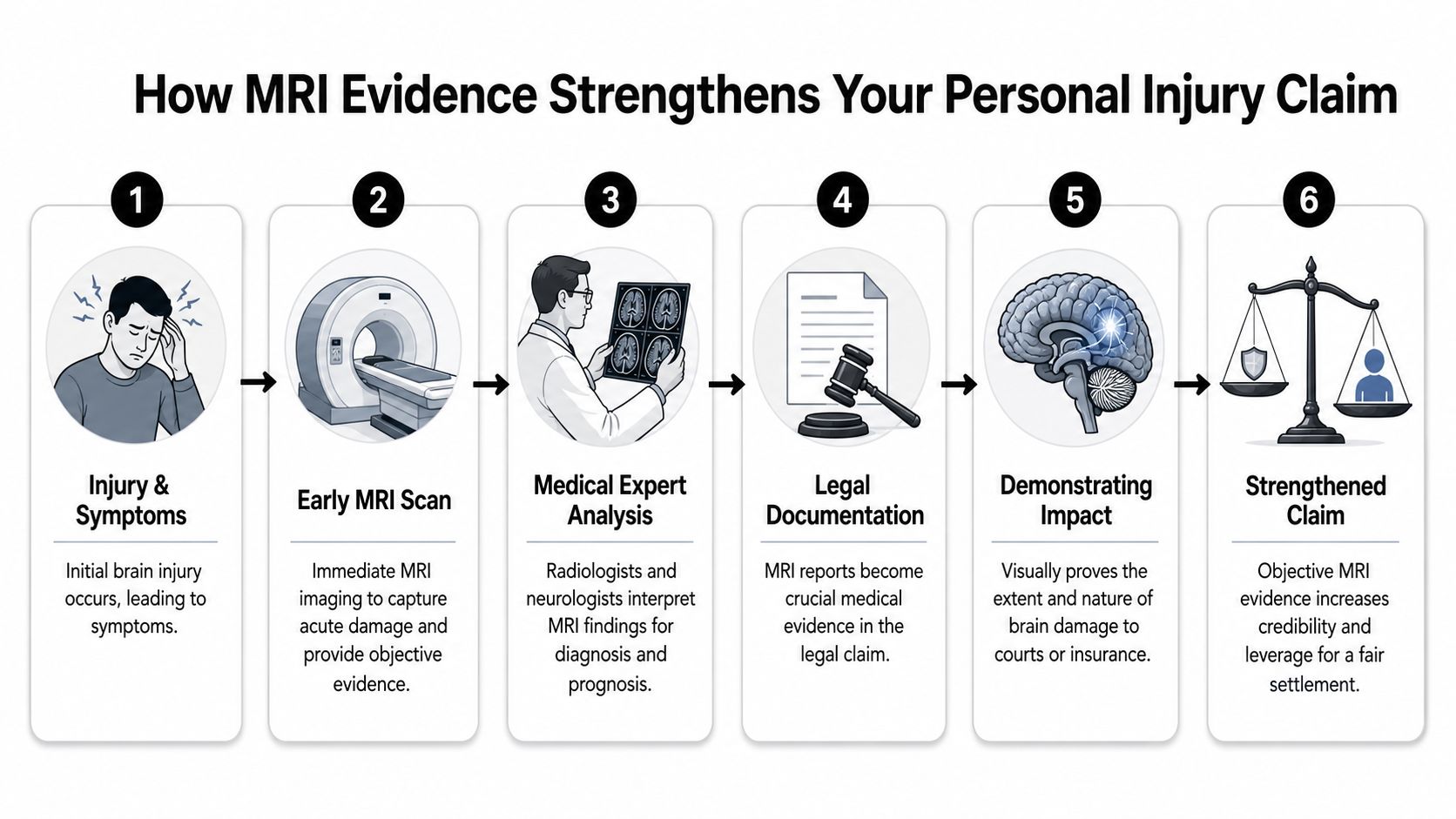
MRI helps prove causation
Causation means linking the injury to the event. In plain language, your legal team must show that the crash, fall, or blow to the head caused the brain injury.
MRI findings can help tie the timing and pattern of injury to trauma. When a radiologist documents contusions, microhemorrhages, or other trauma-consistent abnormalities, those findings can support the argument that the incident was not minor and that the symptoms have a physical basis.
That matters even more when the insurer is relying on the first ER records.
MRI helps show severity
A positive MRI can undercut the defense claim that this was “just a bump on the head.” It can also help explain why a person who looked stable in the emergency room later struggled at work, at home, or in daily life.
Recent hospital data adds another layer to that point. In a 2024 study, hospitalized TBI patients who received an inpatient brain MRI had a lower inpatient mortality rate of 0.75% compared with 2.54% in patients who did not receive MRI, as reported in this study on inpatient MRI and mortality in traumatic brain injury. That does not mean MRI guarantees better long-term recovery, but it does show that MRI is tied to important clinical decision-making in serious cases.
MRI supports future damages
Brain injury cases are rarely just about the first few weeks. The primary fight is often over the future.
A lawyer may use MRI evidence alongside treating physician opinions, neuropsychological testing, and day-in-the-life evidence to argue for:
- Ongoing medical care such as neurology visits, rehabilitation, headache treatment, or counseling
- Loss of earning capacity if concentration, fatigue, or processing speed limit work
- Pain and suffering tied to persistent cognitive and emotional changes
- Loss of normal life when relationships, independence, and daily function have changed
Why the scan itself matters, not just the report
In many cases, the written report is only the starting point. The actual image set can be reviewed again by specialists. A neuroradiologist or other expert may identify findings that become central to the case narrative.
That is why MRI evidence is more than a medical formality. In the right case, it becomes one of the clearest ways to answer the insurance company's favorite question: “Where is the proof?”
Practical Steps to Take for Your TBI MRI
If you think you may need a traumatic brain injury MRI, details matter. The scan should not be treated like a box to check.
First, talk to your doctor about why your symptoms continue. Be concrete. Say when they started, how often they happen, and how they affect work, driving, sleep, and daily tasks. Specific symptom descriptions help providers justify imaging and choose the right protocol.
What to ask for
The technical side matters more than most patients realize. According to federal guidance for diagnostic mild TBI imaging, a diagnostic mTBI MRI requires at least a 1.5 Tesla magnet and should include 3D T1/T2, FLAIR, DWI, and SWI, and for SWI, distortion correction filters should be disabled to maximize microhemorrhage detection, as stated in this government guidance on MRI specifications for mild traumatic brain injury.
You don't need to say that like a radiologist. You can say it like this:
“My CT was normal, but my symptoms haven't resolved. Can you order a brain MRI with a protocol appropriate for traumatic brain injury, including SWI if available?”
What to collect after the scan
Don't leave with only a portal summary if you can avoid it. Ask for:
- The radiology report so you can read the formal interpretation
- The image disc or digital files because specialists may want to review the actual scan
- Visit notes from the ordering doctor that connect the imaging request to your symptoms
- A symptom timeline you keep yourself, updated regularly
If your records are already piling up, a simple system helps. This guide on how to organize with Family Folder offers a practical way to keep imaging reports, discs, appointments, and symptom notes in one place.
What to do for your legal case
Share the MRI report and image files with your attorney promptly. Timing matters. So does context.
A lawyer handling a brain injury case will want to compare the MRI with the ambulance records, ER chart, neurology visits, rehabilitation notes, and your ongoing symptom history. The goal is to build a single, consistent story from injury through recovery.
If the MRI is positive, that evidence should be preserved and interpreted carefully. If it is negative, the case should still be developed through symptoms, treatment history, witness accounts, and expert analysis. Either way, careful documentation protects both your health and your claim.
If you or a loved one is dealing with persistent symptoms after a head injury, Nares Law Group LLC can help you understand how medical imaging fits into a personal injury case. The firm works with injured families facing crashes, truck wrecks, and traumatic brain injuries, and helps clients preserve evidence, coordinate treatment, and push back when insurance companies misuse “normal” scans to deny real harm.